
Code Green Solutions

There is a growing movement to refocus building design and operations on human health. LEED v4 is seeking a market transformation by incorporating materials transparency into its materials and resources credits, and by integrating other health-based strategies into other credit categories, such as indoor environmental quality and energy and atmosphere. (See Worden, Trowbridge, and Pyke; Research Preview: Review of Health Language in LEED). While it’s relatively simple to measure the effectiveness of energy efficiency strategies, the metrics associated with health are much more complex. The large population, multi-year epidemiological studies required to determine the health impacts of hazardous and toxic ingredients, are not feasible for the building industry needs. So how do we measure success in health improvements in buildings in a feasible time-frame? This is critical so that the building industry knows that their strategies are successfully achieving improved occupant health.
The development of health-based metrics for buildings currently is a hot research area. Ideally the best metrics will be easy to measure, truly relatable in real-time to optimized building design, and will incorporate operational strategies that include greener, healthier building materials. The “old ways” of measuring health outcomes included assessing absenteeism rates, particularly in schools, or monitoring asthma exacerbation rates among children by tracking rescue medicine usage. But these metrics, while simple to measure, ignore that there are multiple reasons for absenteeism, many of which are not relatable to building design and operations strategies.
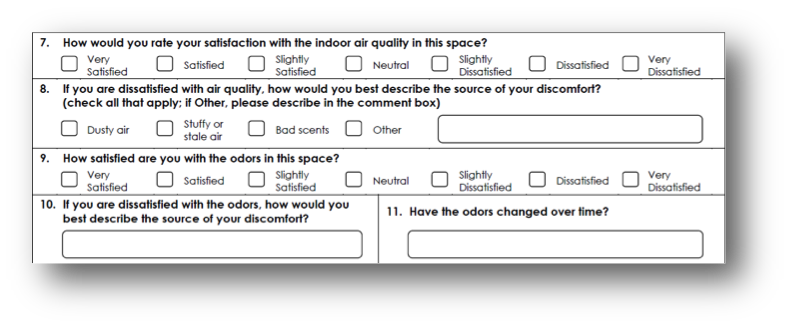
Figure 1. Example of a post-occupancy questionnaire.
Judith Heerwagen, a program expert at the Government Services Administration (GSA), and Esther Sternberg, a professor at the University of Arizona, Tucson, are successfully making direct health measurements in GSA buildings by using heart rate variability and cortisol levels as a measure of stress. The concept is that poor indoor environments cause stress, which is then measureable by these two parameters. Comparisons of these measurements on a group of GSA employees initially working in an older office building and then relocated to a newer, “healthier” office space demonstrated that the employees experienced lower stress levels in the newer office space. Other researchers, including Mark Rea and Mariana Figueiro, both professors at the Lighting Research Center at Rensselaer Polytechnic Institute, are investigating how circadian rhythm can be disrupted by imperfect lighting, impacting sleep quality, and thus concentration and health. Cortisol levels, as well as behavior and health, also were used in a Swedish study (Kuller and Lindsten 1992) of elementary students to track hormonal impacts from daylighting levels on concentration and cooperation.
Questionnaires are another tool frequently used to assess health-related impacts. Post-occupancy questionnaires are used to determine self-reported health symptoms and occupants’ satisfaction with the indoor environment. In particular, they have been used by researchers at the Berkeley Center for the Built Environment to measure satisfaction with mixed-mode and natural ventilation strategies, thermal comfort, and other factors related to the indoor environment (Figure 1). Perception based primarily on odor as a measure of comfort is another type of metric that is being used. The LEED Indoor Air Quality Performance Pilot Credit includes this type of survey as well as air monitoring to determine the success of ventilation and air cleaning strategies in a building. Another type of questionnaire or testing process that is being used that is not really a health metric, but often is being used as such, is to measure task performance. This usually is done by administering a test including specific timed tasks measuring parameters such as recall, matching, typing speed, or analysis. The reliability and effectiveness of task performance/learning tests at measuring human impacts from the indoor environment are dependent their appropriateness at measuring tasks requiring increased concentration, such as clear thinking and symbolic manipulation. Wargocki and Wyon (Wargocki, Wyon, and Fanger 2004; and Wargocki, and Wyon 2006) have found that negative effects of the indoor environment may effect adults’ performance as much as 10% in office buildings and children’s performance more than 20%. However, if these tests are not properly designed or administered, they may not provide valid data. For example, if the tests, particularly when given to children, are repeatedly administered, learning occurs resulting in artificially increased scores and underestimation of the environmental impacts. The direct correlation of these tests to health is yet to be determined, but it can be assumed that improved health will improve concentration and improve performance.
These health metrics are primarily still research tools rather than widely applicable tools for the building industry at this time; however, they are a start in meeting the need. With the exception of carefully designed research studies, it is not possible with these metrics to differentiate which strategies or improved materials are improving health since several different strategies are commonly applied in a building. Nevertheless, the metrics are a step forward to being able to measure the success of approaches to health-focused buildings including greener materials usage. These metrics are different from long-term epidemiological and toxicity studies. They not only measure in a different timeframe, but also are evaluating the indoor environment based on exposures, sick building type symptoms, and softer measures of stress and psychology. Stress and concentration are strongly impacted by indoor environmental factors such as daylighting and access to views, as well as toxic exposures from materials and ventilation rates. It is important to remember that the indoor environment and all aspects of the building are an interactive system, and that multiple improvements, including selection of healthier building materials, will impact occupants’ health. Therefore, measurements of stress and concentration will provide health impact data on all aspects of the improved indoor environment. Additional applications of these health metrics focusing on not only collecting additional data, but designing them for use by the building industry to measure success are next steps necessary to allow for determining the most successful strategies for optimizing health in the built environment.











{kind=link}